AI Route Planning: What Actually Works in DME
Cutting through the hype around AI route optimization. What does it really do for DME delivery and service, and why is it different from routing a pizza fleet?
"AI-powered route optimization" has become a buzzword that every field service vendor throws around. But in DME and respiratory care, routing isn't a generic problem. The constraints are fundamentally different from delivery logistics or HVAC service calls, and most AI routing tools were never designed to handle them. Here's what actually matters when you're routing DME field operations, and what to look for in a solution.
DME Routing Is Not Pizza Delivery
Generic route optimization solves one problem: minimize drive time across a set of stops. That works great when every driver can serve every stop and the only variable is distance. In DME, the problem is far more constrained. A respiratory therapist credentialed with one payer can't be assigned to a patient covered by a different payer. A technician certified for oxygen setups shouldn't be routed to a complex ventilator delivery. A driver without a CDL can't operate certain vehicles.
These aren't edge cases. They're the core reality of DME field operations. Any routing system that doesn't understand credential matching, equipment competency, and payer requirements will generate routes that look efficient on paper but fall apart in the field.
What Real AI Routing Does
Effective AI route planning for DME handles multiple constraint layers simultaneously:
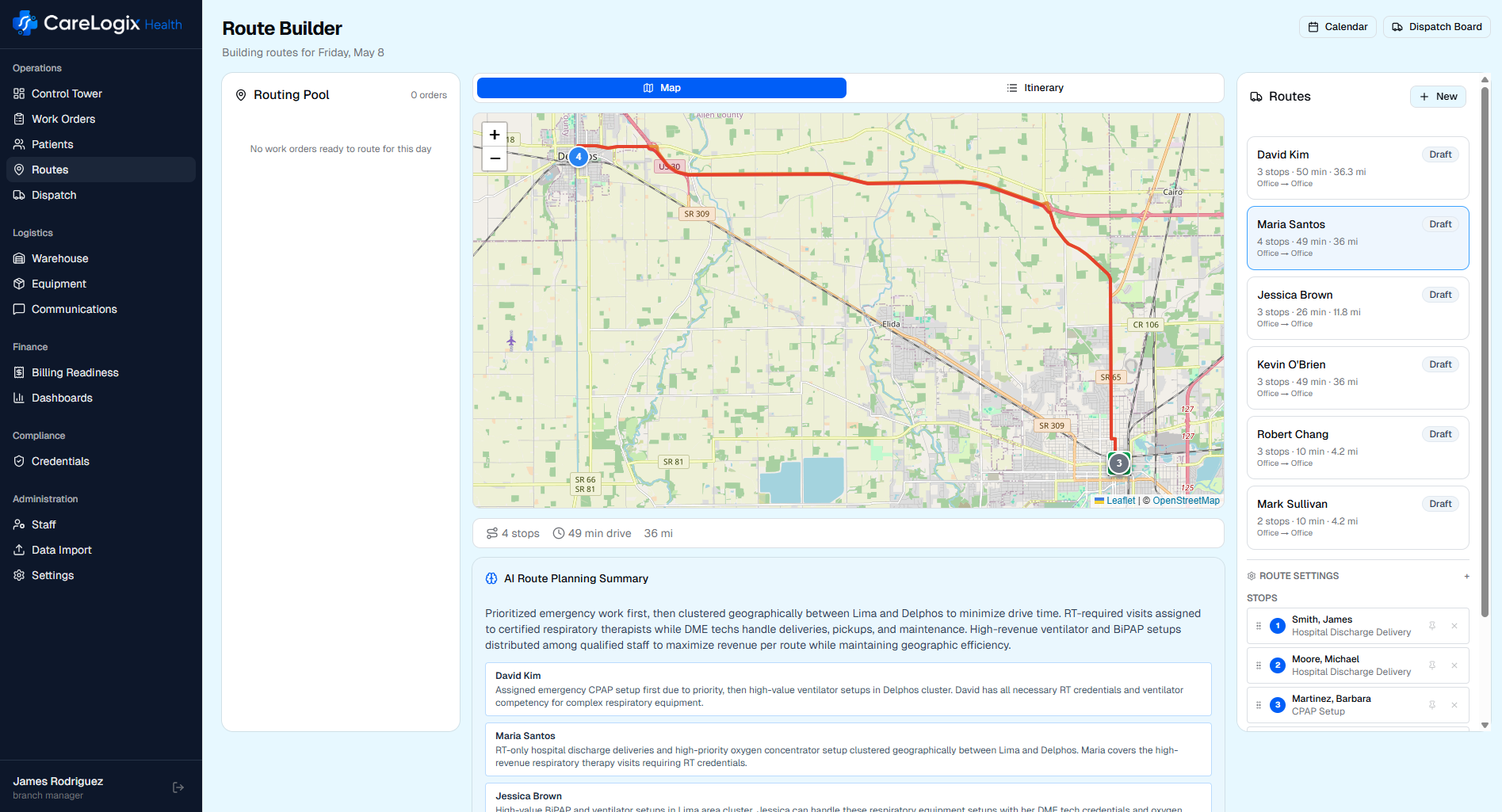
- Credential matching: The system knows which technicians are credentialed with which payers and only assigns them to eligible patients.
- Equipment competency: Complex setups like ventilators or enteral nutrition require specific training. The system respects these requirements.
- Geographic clustering: Rather than optimizing a single route in isolation, AI groups stops into geographic clusters first, then optimizes within each cluster. This prevents the common problem of technicians zigzagging across a service area.
- Workload balancing: Routes aren't just about minimizing miles. They need to balance appointment complexity, setup time, and total hours across the team.
- Real road data: Straight line distance between two points is meaningless in a metro area where a river, highway closure, or one-way street pattern can triple actual drive time. Proper routing uses real road network data and traffic patterns.
The Difference Between "Optimized" and "Feasible"
Many routing tools will produce a mathematically optimal route that is operationally infeasible. The shortest path might send a tech to a patient whose insurance they aren't credentialed for. The most "balanced" distribution might overload your only vent-certified RT while leaving general delivery techs idle.
Good AI routing in DME starts with feasibility, meaning every stop is assigned to someone who can actually serve it, and then optimizes within those constraints. This is a harder problem computationally, but it's the only approach that produces routes dispatchers don't have to manually rebuild every morning.
What Results to Actually Expect
Vendors love to claim 30% or 40% reductions in drive time. Those numbers are possible if you're coming from completely manual dispatching with no geographic logic at all. For most DME providers who already have decent dispatchers, realistic improvements look more like this:
- 10-20% reduction in total daily miles driven
- 1-2 additional stops per technician per day through better sequencing
- Near-zero credential mismatches on initial route generation
- 70-80% reduction in morning route adjustment time for dispatchers
- Faster recovery from mid-day disruptions like cancellations, add-ons, or vehicle breakdowns
These are meaningful operational improvements. An extra stop per tech per day across a 50-person field team adds up to 250 additional patient visits per week. That's real revenue and better patient access.
The Bottom Line
AI route planning works in DME, but only when it's built for DME. If your routing tool doesn't understand payer credentials, equipment competencies, and healthcare-specific scheduling constraints, you're using a solution designed for a different industry. The results will reflect that gap.
The best route isn't the shortest one. It's the one where every technician is qualified for every stop, every patient gets served on time, and your dispatchers didn't have to rebuild it by hand.
About the Author

Adam Donaldson
Founder, CareLogix Health
Adam built CareLogix after years of implementing field operations systems at enterprise DME providers. He saw firsthand how fragmented tools, manual processes, and disconnected workflows cost branches hours every day and leak revenue that should have been captured. CareLogix is the platform he wished existed when he was on the implementation side.
Connect on LinkedInSee CareLogix in Action
Schedule a 30-minute walkthrough and see how CareLogix manages the full work order lifecycle for DME providers like you.